December Informed Newsletter 2022
December 20, 2022Wishing You the Best This Holiday Season
As we celebrate the close of one year and the start of another, we want to thank you for all the world-class care you’ve provided our members throughout 2022. Your partnership is a gift we’re truly grateful for this holiday season. We hope you and your staff – and your family, friends and loved ones – have an abundance of blessings, joy and good health. Thank you, as always, for all that you do.
As It Relates to You
Key information for you and your staff.
Continued Gratitude – A Note of Thanks from
Your Provider Relations Team
From your Provider Relations staff, we wish you all a happy, healthy and prosperous New Year. Each day, you give your patients one of the most important gifts of all – the best health and livelihood possible. Thank you for your constant, tireless, wonderful efforts!
Please Remind Your Patients to Get Their Flu Shots
As healthcare providers, you know how important flu shots are to your patients, their families and the community in general. This winter – like the last two – they’re more essential than ever due to the ongoing COVID-19 pandemic. Flu shots are especially important for those at high risk from influenza, many of whom are also at high risk for contracting COVID-19 or developing serious outcomes if they do.
Remind your patients that it’s not too late to get their flu shot. It varies according to health plan, but flu shots are covered at no cost to the member in most cases. Your patients can call the number on the back of their health plan member ID card to learn more about costs and where they can go to get their vaccinations. Together we can help keep our community healthy and well this winter.
***
Help Us Move the Needle
Together we can help people live their healthiest lives. Find reminders, tips and more in this section, to guide improvements in patient outcomes. Help us move the needle.
Dual Diagnosis – Key Information You Should Know
Do you know what “dual diagnosis” is? Here’s the key information, from MedlinePlus.
Dual Diagnosis – What is it?
A patient with a dual diagnosis has both a mental health disorder and a drug or alcohol problem. It’s very common for these conditions to occur together, and their interactions with one another can worsen both conditions.
Why do they often occur together?
Even though mental health and substance use disorders often occur together, that doesn’t necessarily mean one caused the other. Experts believe there are three general reasons why they might frequently occur together:
- A patient may have risk factors – such as genetics, stress or trauma – that contribute to both mental health and substance use disorders.
- Mental health disorders can contribute to substance use – and to substance use disorders. Some people with mental health issues use drugs or alcohol to temporarily feel better. Also, some mental health disorders can change the brain, making it more likely for someone to become addicted to substances.
- Substance use – and addiction – can contribute to the development of mental health disorders. It can change the brain in ways that make someone more likely to develop mental health issues.
How is dual diagnosis treated?
You must treat both conditions. And the patient needs to stop using the drugs or alcohol. Effective treatments can include behavioral therapies and medications. Many patients also benefit greatly from support groups, where they can get the emotional and social support they need.
Help Promote Foot Health for Your Patients with Diabetes
Foot issues can cause many problems for people with diabetes – but podiatrists and other providers can help with early detection of problems, awareness raising, treatment and more. Here’s key information from the CDC.
The Basics
Yearly comprehensive foot exams, and treatment if needed, can help your patients avoid or delay nerve damage (neuropathy), blood vessel damage (vasculopathy), joint damage (arthropathy) and more. These exams should include an evaluation of foot structure and function, pulses, sensation and the person’s nails.
Share These Key Messages with Your Patients
- Remind your patients to ask for a basic foot check at every single healthcare visit they have.
- Give your patients the knowledge they need. Inform them that:
- Diabetes-related complications can start in the feet.
- These potentially harmful complications often have no recognizable symptoms.
- But getting a basic foot check at every healthcare visit, along with their yearly comprehensive foot exam, can help detect issues early.
- People with poorly managed blood sugar or high blood pressure may benefit from comprehensive foot exams every three or six months, rather than getting just one yearly.
Five Actions the CDC Recommends for Providers
- Recognize the risks of foot issues and amputation for your patients with diabetes.
- Know how diabetes can affect foot health – and tell your patients to watch for:
- Burning, tingling or numbness – or the feeling of “bugs crawling on their skin.”
- Redness, wounds, ulcers or new foot pain.
- Calluses, corns, nail deformities or bleeding beneath the nails.
- Foot swelling, newly walking with a limp, changes in foot shape or shoes no longer fitting.
- At every visit: ask your patients questions about their foot health.
- Help keep your patients’ blood sugar, blood pressure and blood lipids at healthy levels.
- Refer your patients to diabetes – and foot-care – self-management information, resources, education, tools and support services.
With your help, your patients with diabetes can keep their feet healthy for the years ahead. Thank you.
Migraine Prevention Treatment – Key Things to Know
Is preventive treatment for migraines right for your patients? If so, how can you choose the right type or types of treatment? What else should you know? Here’s the key information from the American Headache Society.
When should preventive treatment be considered and/or offered?
In general, when your patient:
- Has four or more migraine-days a month.
- Is significantly debilitated by their migraines, even if they’re infrequent. For example, as with hemiplegic migraines or migraines with brainstem aura.
- Has experienced failure or overuse of acute therapies and the risk of medication overuse.
- Wants to pursue a preventive treatment option.
What are the goals of preventive treatment?
- Lower the number of migraines.
- Reduce migraine-days and headache-days.
- Ease symptom severity.
- Decrease migraine-related disabilities.
- Reduce acute medication use.
What are the main principles of preventive treatment?
- Get to know your patient – understand their goals and preferences (such as natural approaches vs. medications) for treatment.
- Set realistic expectations for your patients – for example, reduction in the number and severity of migraines, vs. complete elimination of them.
- Distinguish between episodic vs. chronic migraines.
- Pick treatments that evidence has proven are most effective. And always consider the side effects of each option.
- Start with lower doses and increase (if needed) slowly.
- Know that improvement is gradual – give each treatment at least two months to see if it’s working.
- Know your patients’ comorbidities – and choose medications that can treat coexisting disorders if possible.
- Consider the costs of each treatment option – and also any insurance restrictions or barriers.
- If a treatment is only partially effective, possibly consider a combination of preventive treatments.
References Used for This Article
Nada Hindiyeh, MD, “How Do I Help My Patient Choose the Right Preventive Treatment?,” First Contact: Headache In Primary Care, American Headache Society.
Guidelines and Best Practices for Statin Therapy Treatment
As you likely know, statins are lipid-lowering medicines that can help reduce illness and mortality for those at high risk of cardiovascular disease. They’re used by many people to help lower their cholesterol.
Following the 2013 guidelines of the American College of Cardiology and the American Heart Association, statins are recommended:
- For people with diabetes age 40 to 75 with LDL-C ≥ 70mg/dL, for primary prevention.
- For these individuals, moderate- or high-intensity statins are recommended. Low-intensity options are also permitted, since some people may experience statin-related side effects.
- For people with clinical atherosclerotic cardiovascular disease (ASCVD), for secondary prevention.
- For these individuals, high-intensity statins are recommended. Moderate-intensity options are also permitted, since some people may experience statin-related side effects.
Rather than aiming for a specific LDL-C target, these guidelines emphasize lowering ASCVD risk with the maximum tolerated statin intensity. Intensity depends on the percent change in LDL-C from baseline, rather than absolute LDL-C reduction. Evidence supporting these guidelines and recommendations includes the following:
- For adults with diabetes without cardiovascular disease, moderate-dose statin therapy lowered the risk for cardiovascular events by over 25% per 38.7mg/dL LDL-C reduction.
- For adults with heart disease, statin therapy lowered the risk for cardiovascular events by over 20% per 38.7mg/dL LDL-C reduction.
- For both adults with and without cardiovascular disease who received more intensive statin therapy or statins compared with a placebo, the risk for cardiovascular disease mortality was lowered by almost 15% per 38.7mg/dL LDL-C reduction.
Antibiotics – They’re Not Always the Right Solution for Children
Antibiotics are not appropriate for every situation. In fact, overprescribing of these medicines can cause real harm. According to recent evidence, children inappropriately given antibiotics were at higher risk of Clostridioides difficile infections and allergic reactions.
In one study of nearly 3 million U.S. children, providers inappropriately prescribed antibiotics – for example, giving antibiotics for viral infections or prescribing non-first-line antibiotic therapy for bacterial infections – in up to 70% of viral upper respiratory infection cases and one-third of bacterial infection cases. And real harm resulted:
- Inappropriate prescribing for bacterial infections was linked with a sixfold greater risk for Clostridioides difficile infections, a fourfold higher risk for severe allergic reactions and an excess risk for gastrointestinal symptoms including diarrhea.
- Improper prescribing for viral infections was linked with excess risk for skin rash.
Often, providers might be asked, or even pressured, by parents to give their children antibiotics (simply because the parents don’t know what’s best in these situations). Perhaps the best approach? Have a friendly, open discussion with the parents about risks vs. benefits. Rather than saying something like, “the guidelines recommend…,” instead perhaps take this approach: “The antibiotics probably won’t help the ear pain get better any quicker – and I’m worried they might cause your child to have diarrhea.” Usually, parents aren’t even aware of the possible side effects, and they’ll appreciate your knowledge, openness and care looking out for their child.
References Used for This Article
James A. Feinstein, MD, MPH, “What Are the Consequences of Inappropriate Antibiotic Prescribing for Pediatric Outpatients?,” Informing Practice, 23 June 2022.
***
Coding Counts:
2023 ICD-10 Updates for
Documenting and Coding Dementia
Supporting documentation and accurate coding are key to making sure your patients receive the care they need. Failure to document persisting conditions on an annual basis impacts your patients, fellow providers and our organization. We’re here to help. Here’s the latest important coding information: ICD-10-CM has updated guidelines and added diagnosis codes for reporting dementia.
New diagnosis codes for dementia that is present in other conditions include etiology, severity and associated conditions. Use of these expanded code sets allows for specificity and a comprehensive understanding of the patient’s health status.
| Expanded ICD-10-CM Codes | Severity | Associated Condition |
| F01.50-F01.C4 Vascular Dementia | Mild | Agitation |
| F02.80-F02.C4 Dementia in Other Diseases | Moderate | Anxiety |
| F03.90-F03.C4 Unspecified Dementia | Severe | Mood Disturbance |
| Unspecified | Psychotic Disturbance |
When reporting Dementia in Other Diseases Classified Elsewhere (F02.80-F02.C4), also report the underlying condition. For example:
G20 – Parkinson’s disease.
F02.B11 – Dementia in other diseases classified elsewhere, moderate, with agitation.
When the etiology for the patient’s dementia is unknown, Unspecified Dementia (F03.90-F03.C4), severity and associated conditions can still be reported. For example:
F03.A3 – Unspecified dementia, mild, with mood disturbance.
New and updated codes for mild cognitive impairment (MCI), so stated:
- Revised: G31.84 – Mild cognitive impairment of uncertain or unknown etiology.
- New: F06.70 – Mild neurocognitive disorder due to known physiological condition without behavioral disturbance.
- New: F06.71 – Mild neurocognitive disorder due to known physiological condition with behavioral disturbance.
Code assignment should be made based on the provider’s clinical judgement and documentation as defined in the ICD-10-CM Official Guidelines for Coding and Reporting.
We thank you for your exceptional professionalism and attention to detail, and we’re here to help. To find more coding resources, visit our Coding Counts page. Thank you for your continued care and dedication to our members’ health.
Questions?
Please contact us at CodingCounts@HealthAlliance.org.
References Used for This Article
ICD-10-CM Official Guidelines for Coding and Reporting
Optum EncoderPro
Centers for Medicare & Medicaid Services
Some Services Will No Longer Require
Prior Authorization in 2023
We know how busy you are, and we’re always working hard to try to find ways to make your jobs a little bit easier. Earlier this year, we announced the removal of prior authorization requirements for ultrasound imaging tests from our Standard Prior Authorization list. These changes included removal of prior authorization for general and obstetric ultrasounds, with some limited specialty ultrasounds continuing to require prior authorization. These modifications around ultrasound imaging tests will carry into the upcoming year and apply to our 2023 Standard Prior Authorization list.*
We’re also happy to report that in 2023, we’ll no longer require prior authorization for an additional three services or durable medical equipment (DME): non-urgent ground ambulance, oxygen and manual wheelchairs. These will be removed from our 2023 Standard Prior Authorization list effective January 1, 2023. Air ambulance and electric or motorized wheelchairs will continue to require prior authorization.
We hope you’re as excited as we are about these changes. We’ve listed the removed oxygen and wheelchair CPT below. Non-urgent ground ambulance claims will be adjudicated through our internal process.
As we look to keep serving you better, we’re committed to modifying our prior authorization list through a data-driven approach, evidence-based care recommendations, and feedback from you and your patients. If you have questions, please contact your provider relations specialist.
*Please log in to Provider.HealthAlliance.org to perform a member plan-specific search to determine whether specific CPT and HCPCS codes require prior authorization, or please contact your provider relations specialist.
Oxygen Codes No Longer Requiring Prior Authorization
| E0425 | DME | OXYGEN |
| E0430 | DME | OXYGEN |
| E0431 | DME | OXYGEN |
| E0435 | DME | OXYGEN |
| E0440 | DME | OXYGEN |
| E1390 | DME | OXYGEN |
| E1391 | DME | OXYGEN |
| E1392 | DME | OXYGEN |
| K0738 | DME | OXYGEN |
Manual Wheelchair Codes No Longer Requiring Prior Authorization
| K0001 | DME | WHEELCHAIRS |
| K0002 | DME | WHEELCHAIRS |
| K0003 | DME | WHEELCHAIRS |
| K0004 | DME | WHEELCHAIRS |
| K0005 | DME | WHEELCHAIRS |
| K0006 | DME | WHEELCHAIRS |
| K0007 | DME | WHEELCHAIRS |
| K0008 | DME | WHEELCHAIRS |
| E1039 | DME | WHEELCHAIRS |
| E1161 | DME | WHEELCHAIRS |
| E1231 | DME | WHEELCHAIRS |
| E1233 | DME | WHEELCHAIRS |
| E1234 | DME | WHEELCHAIRS |
| E1235 | DME | WHEELCHAIRS |
| E1236 | DME | WHEELCHAIRS |
| E1237 | DME | WHEELCHAIRS |
| E1238 | DME | WHEELCHAIRS |
| E2230 | DME | WHEELCHAIRS |
| E2616 | DME | WHEELCHAIRS |
Partnering With eviCore to Introduce Radiology and Chemotherapy Bundling Enhancement
Together with eviCore, we’re continually working to enhance your prior authorization experience and our processes. EviCore recently implemented efficiencies around the request for imaging authorizations throughout the surveillance of a patient’s chemotherapy treatment. Here’s what you should know.
What is it?
- This bundling initiative is a process of creating an authorization for multiple, ongoing, diagnostic imaging studies at the point of first request for diagnostic imaging, where chemotherapy has already been approved by eviCore. The radiology cases are approved based on a grouping of oncology variables/inputs for a member’s condition.
Why We Need It
- To reduce provider burden by eliminating the need for the provider to request imaging authorizations throughout the surveillance of a patient’s chemotherapy. Instead of having to request each diagnostic imaging study individually (for each DOS), one authorization will cover 12 months of the appropriate imaging.
What’s in Scope (See Appendix)
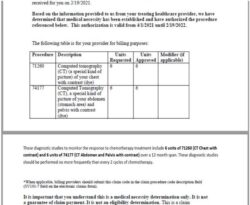
- 70553 (MRI Brain With and Without Contrast) is approvable, without clinical review, when CHEMO request is for Central Nervous System and includes appropriate diagnosis code and “Subtype” is Anaplastic Gliomas/Glioblastoma.
- 71260 (CT Chest With Contrast) and 74160 (CT Abdomen With Contrast) are approvable, without clinical review, when CHEMO request is for Stage 4 Non-Small Cell Lung Cancer and includes appropriate diagnosis codes.
- 71260 (CT Chest With Contrast) and 74177 (CT Abdomen and Pelvis With Contrast) are approvable, without clinical review, when CHEMO request is for Stage 4 Small Cell Lung Cancer, Breast Cancer, Pancreatic Cancer, Kidney Cancer, Colorectal Cancer and includes appropriate diagnosis codes.
Critical Data Need
- These bundles can only be applied based on distinct member attributes. In order to determine a distinct member, the same patient ID must be used when requesting the diagnostic imaging that was used for requesting the CHEMO authorization. If different patient IDs are used for each of the requests, a bundle will not be presented when requested.
How It Works
- Upon approval of chemotherapy that meets the criteria for the scope of this bundling initiative, approval language will be included in the chemotherapy authorization indicating if the bundle is available.
- If a provider makes a request for a radiology procedure where eviCore has approved a previous request for chemotherapy (and there is a “bundle allowed” based on criteria above), the pathway will ask:
- “Are you requesting <CPTCode> in order to monitor the response to previously approved chemotherapy?”
- If no, a standard radiology request for one unit will be created and will proceed through the standard review.
- If yes, the radiology case is updated with defined units (total of four to 12), timespan (365 days) and procedure codes (see ruleset in Appendix).
- Standard radiology approval authorizations will be issued with the case basket of procedure codes with approval language addressing the bundle:
- “Are you requesting <CPTCode> in order to monitor the response to previously approved chemotherapy?”
As always, if you have any questions, you can contact your provider relations specialist. They’ll be more than happy to help.
Appendix: Governing Ruleset
- Defines if chemotherapy request presents in a way that allows radiology surveillance authorizations to be auto-created:
| Location | Subtype | ICD9 Code | Current Stage Code | Diagnostic CPT Code | Paired CPT Code | Post Approval | Timeframe | Initial Units | Subsequent Units | Eligible | |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.0 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.1 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.2 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.3 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.4 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.5 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.6 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.7 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.8 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOCNS | * | Anaplastic Gliomas/Glioblastoma | C71.9 | * | 70553 | NotFound | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.00 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.01 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.02 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.10 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.11 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.12 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.2 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.30 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.31 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.32 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.80 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.81 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.82 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.9 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.90 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.91 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOSCLC | * | * | C34.92 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.00 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.01 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.02 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.10 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.11 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.12 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.2 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.30 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.31 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.32 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.80 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.81 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.82 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.9 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.90 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.91 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MONSCL | * | * | C34.92 | 4 | 71260 | 74160 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.011 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.012 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.019 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.021 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.022 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.029 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.111 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.112 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.119 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.121 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.122 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.129 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.211 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.212 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.219 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.221 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.222 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.229 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.311 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.312 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.319 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.321 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.322 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.329 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.411 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.412 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.419 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.421 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.422 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.429 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.511 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.512 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.519 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.521 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.522 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.529 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.611 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.612 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.619 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.621 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.622 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.629 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.811 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.812 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.819 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.821 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.822 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.829 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.911 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.912 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.919 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.921 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.922 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOBREA | * | * | C50.929 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.0 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.1 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.2 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.3 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.4 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.7 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.8 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOPANC | * | * | C25.9 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MORENA | * | * | C64.1 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MORENA | * | * | C64.2 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MORENA | * | * | C64.9 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.0 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.1 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.2 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.3 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.4 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.5 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.6 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.7 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.8 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Colon | * | C18.9 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| MOCOLO | Rectal | * | C20 | 4 | 71260 | 74177 | 42 | 365 | 6 | 4 | Y |
| * | * | * | * | * | NA | NA | NA | NA | NA | NA | N |
New Standard Prior Authorization List for 2023
Click here to view our new Standard Prior Authorization list for 2023, effective January 1, 2023.
Updates to High Cost Medical Drugs List
See the table below for changes to the High Cost Medical Drugs List with effective dates.
Note: Medications removed from the High Cost Medical Drugs List may still require prior authorization.
Note: This article/table does not apply to Medicare plans.
| Drug Therapy | Drug Name | Code | PA | Effective | Preferred
Vendor |
Contact
Number |
Change |
| Oncology – Injectable | CARVYKTI | Q2056 | YES | 10/1/2022 | Hospital Access Only | Added | |
| Acromegaly | LANREOTIDE | J1932 | YES | 10/1/2022 | Optum Specialty | (855) 427-4682 | Added |
| Oncology – Injectable | OPDUALAG | J9298 | YES | 10/1/2022 | Optum Specialty | (855) 427-4682 | Added |
| Blood Modifier | RELEUKO | Q5125 | NO | 10/1/2022 | Optum Specialty | (855) 427-4682 | Added |
| Ophthalmology Disorders | VABYSMO | J2777 | NO | 10/1/2022 | Optum Specialty | (855) 427-4682 | Added |
Midwest Pharmacy Updates
All Plans
Neurology
Formulary Additions
- Amvuttra (vutrisiran)—Treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis (hATTR-PN) in adults
- Formulary placement recommendations
- Commercial—Non-Preferred Specialty Medical with PA
- Medicare—Medicare Part B
- Formulary placement recommendations
- Vabysmo (faricimab-svoa)—Treatment of neovascular (wet) age-related macular degeneration and diabetic macular edema
- Formulary placement recommendations
- Commercial—Non-Preferred Specialty Medical
- Medicare—Medicare Part B
- Formulary placement recommendations
Commercial
Neurology
New Commercial Policies
- Combination Medications for EHB
- Firdapse (amifampridine)
Commercial Criteria Changes
- Cerdelga (eliglustat tartrate)
- Updated with additional exclusion criteria
- Cerezyme (imiglucerase)
- Added age requirement
- Carbaglu (carglumic acid)
- Added ordering prescriber requirement
- Crysvita (burosumab)
- Added new diagnosis and criteria
- Updated approval period
- Lumizyme (alglucosidase)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Nexviazyme (alglucosidase alfa-ngpt)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Naglazyme (galsulfase)
- Added gene testing requirement
- Mepsevii (vestronidase alfa-vjbk)
- Added exclusions
- Makena (hydroxyprogesterone caproate)
- Added generic to policy
- Added criteria for generic for non-pregnancy related indications
- Onpattro (patisiran)
- Added Amvuttra to policy
- Updated approval period
- Tegsedi (inotersen)
- Added Amvuttra to disallowed concurrent medications
- Enspryng (satralizumab)
- Added exclusion criteria
- Uplizna (inebilizumab)
- Added clarification that Uplizna will not be approved for use in combination with Enspryng or Soliris
- VPRIV (velaglucerase alfa)
- Added Zavesca to disallowed concurrent medications
- Zavesca (miglustat)
- Updated coverage criteria
- Updated age requirement
- Hereditary Angioedema
- Updated Orladeyo MDL
- Spinraza (nusinersen)
- Added medical director review requirement
- Updated approval period
- Vimizim (elosulfase alfa)
- Added required evidence of specific gene mutation
- Kuvan (sapropterin)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Updated approval periods
- Orfadin (nitisinone) and Nityr (nitisinone)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Samsca (tolvaptan)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Syprine (trientine hydrochloride)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Emflaza (deflazacort)
- Updated approval period
- Galafold (migalastat)
- Updated approval period
- Givlaari (givosiran)
- Updated criteria and approval period
- Keveyis (dichlorphenamide)
- Updated approval period
- Oxlumo (lumasiran)
- Updated approval period
- Palynziq (pegvaliase-pqpz)
- Updated approval period
- Revcovi (elapegademase)
- Updated approval period
- Strensiq (asfotase alfa)
- Updated approval period
- Zokinvy (lonafarnib)
- Updated approval period
Additional Commercial Criteria Changes
- Crohn’s Policy
- Added Skyrizi
- Diabetes Policy
- Removed Mounjaro-specific section and added Mounjaro to GLP-1 section
- Clarified that GLP-1 products will be approved for FDA-approved indications and not solely for weight loss
- Atopic Dermatitis Policy
- Removed Eucrisa step in section 1
- Added step through preferred products in section 2
- Ankylosing Spondylitis Policy
- Added Enbrel to preferred products
- Plaque Psoriasis Policy
- Added Enbrel to preferred products and Sotyku to non-preferred products
- Psoriatic Arthritis Policy
- Added Enbrel to preferred products
- Polyarticular Juvenile Arthritis Policy
- Added Enbrel to preferred products
- Rheumatoid Arthritis Policy
- Added Enbrel to preferred products
Retired Policies
- Korsuva (difelikefalin)
- Will be bundled with other dialysis products
- Ruzurgi (amifampridine)
- Drug is discontinued
Tier Changes
Commercial
Positive Changes
- Alphagan P: Move from Non-Preferred Brand to Preferred Brand
- Cibinqo: Move from Non-preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Combigan: Move from Non-Preferred brand to Preferred brand
- Simbrinza: Move from Non-Preferred brand to Preferred brand
- Enbrel: Move from Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy (effective 1/1/23)
- Firdapse: Move from Excluded to Non-Preferred Specialty Pharmacy
- Kerendia: Move from Non-Preferred Brand to Preferred Brand
- Lanreotide: Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Mounjaro: Move from Non-Preferred Brand to Preferred Brand
Negative Changes—Effective 1/1/2023
- Betoptic- S: Move from Preferred Brand to Non-Preferred Brand
- Tecfidera: Move from Preferred Specialty Pharmacy to Non-Preferred Specialty Pharmacy
Medicare
Medicare Part D Policies
- New policy: Medicare D Ztalmy
- Criteria changes: Medicare D Skyrizi
- Added criteria and indication for PsA and Crohn’s disease
2023 Medicare Pharmacy Formulary Changes
Positive Changes
Positive Formulary Additions, Increases
| CHANGE | DRUG |
| Addition | Flovent Diskus and Flovent HFA- Tier 4, ST, QL |
| Addition | Gemtesa – Tier 4 |
| MDL increase | Lidocaine/prilocaine cream- increase QL to 60g/30 days **not on initial
formulary for 9/1 Marcom release |
| Addition | Moxifloxacin 400mg tablets- Tier 2 |
| Addition | Ropinirole ER tablets – Tier 2 |
B V D Changes
| B v D removal | Cabenuva susp |
| B v D removal | Duramorph inj |
| B v D removal | Morphine Sul inj 0.5mg/ml, 1mg/ml, 2mg/ml, 4mg/ml |
Positive Tier Changes
| Tier 5 to Tier 3 | · Dalfampridine 10mg ER tabs |
| Tier 2 to Tier 1 | · Klor-Con M15 15meq ER tabs
· Pot cl micro 15meq ER tabs |
Negative Changes
Remove from the Formulary
| Afinitor tablets (no utilization,
generic available) |
Albuterol tablets (discontinued in U.S > 1
year) |
Ambisome inj
(no utilization, generic available) |
Anadrol-50 tabs (discontinued in U.S > 1
year) |
| Aplenzin tabs (remove brand- generic option
available) |
Apokyn inj (remove brand- generic option available) | Apo-Verenicline tablets (remove brand- generic option
available) |
Aptivus solution (discontinued product, capsules still on
formulary) |
| Arcapta caps (discontinued in U.S > 1 year) | Avandia tablets (discontinued in U.S > 1 year) | Azasan tablets (remove brand-no utilization, generic
available) |
Azopt 1% opth susp (remove brand- 1 member, generic
available) |
| Baciim inj (other generic
options available) |
BYNFEZIA PEN INJ 2500MCG
(discontinued product, other generic available) |
Bydureon 2mg inj pen (discontinued product with BCise product
available) |
Bystolic tabs (remove brand, generic available) |
| Captopril/HCTZ tabs (discontinued in U.S > 1 year) | Carbaglu tabs
(remove brand, generic available) |
Chantix pak and tabs (remove brand, no utilization, generic
available) |
Clovique caps (discontinued product, generic available) |
| Crixivan caps (discontinued product) | Cuvposa soln (remove brand, no
utilization, generic available) |
Didanosine caps (discontinued in U.S > 1 year) | Cystadane powd (remove brand, no utilization, generic
available) |
| Diastat gel (remove brand, no utilization, generic
available) |
Dilantin oral susp (remove brand, no
utilization, generic available) |
Duexis tabs (remove brand, no utilization, generic
available) |
Epaned soln (remove brand, generic available) |
| Epirubicin hcl inj (discontinued product) | Erwinaze inj (discontinued product) | Ferriprox tabs (brand removal, no
utilization, generic available) |
Freamine HBC inj 6.9% (discontinued product,
other generics available) |
| Glycate tabs (remove brand, discontinued product, generic
available) |
Gralise tabs (removed due to pricing, other options available) | Guanidine tabs (discontinued in U.S > 1 year) | Hectorol inj (brand removal, generic available) |
| Hepatamine soln (discontinued product) | Horizant tabs (removed due to pricing, other options available) | Hydrocodone/acetami nophen 10/325mg soln (discontinued
product) |
Intelence 100mg, 200mg tabs (brand removal, no utilization,
generic available NF) |
| Kaletra 100/25mg tabs (no utilization) | Ketoprofen
(IR and ER) caps (no utilization, high cost medication) |
Lanoxin tabs (brand removal, no utilization, generic available) | Lazanda spr (discontinued product) |
| Levorphanol tabs (no utilization, high cost, other alternatives
available) |
Maprotiline tabs (discontinued product) | Mondoxyne NL caps (product discontinued, other generic alternatives available) | Morgidox caps (product discontinued, other generic alternatives available) |
| Namenda XR caps (brand removal, generic alternative
available) |
Nephramine inj (discontinued product) | Nitrostat sl tabs (brand removal, generic available) | Northera caps (brand removal, no utilization, generic
available) |
| Oxycodone/ASA tabs (discontinued in U.S > 1 year) | Pacerone tabs (brand removal, generic available) | Paxil susp
(brand removal, no utilization, generic available) |
PEG-intron kit (discontinued in U.S > 1 year) |
| Pepaxto inj
(voluntary removal from market) |
Phospholine opth soln. (discontinued product) | Prednicarbate 0.1%
cream (discontinued product) |
Propantheline tabs
(discontinued in U.S > 1 year) |
| Propranolol/HCTZ tabs (discontinued product by 6/23, available
separately) |
Revlimid 5mg, 10mg, 15mg, 25mg (brand removal, generic available) | Riomet ER susp (discontinued product) | Selzentry 150mg, 300mg (brand removal, generic available) |
| Sutent caps (brand removal, generic available) | Tolbutamide tabs (discontinued product) | Tolmetin sod caps (discontinued in U.S > 1 year) | Tremfya inj (switching preferred and non-preferred
products) |
| Trilyte soln (discontinued
product) |
Trokendi XR caps (brand removal, generic available) | Utibron caps (discontinued in U.S >
1 year) |
Virt-Nate DHA caps (discontinued product) |
| Xcopri pak
(250mg daily dose) (discontinued product) |
Xpovio pak
(100mg and 40mg packs) (discontinued products) |
Zortress tabs (brand removal, no
utilization, generic available) |
Quantity Limits Added
| Dextroamphetamine 5mg/5ml soln- 1800/30 days |
| Linezolid 100mg/5ml susp- add 1800/30 days |
| Mayzent 0.25mg tabs- 120 per 30 days |
| Mayzent starter pack 0.25mg – 14 per 365 days |
| Mayzent starter pack 0.25mg – 24 per 365 days |
| Mayzent 1mg tabs – 30 per 30 days |
| Mayzent 2mg tabs – 30 per 30 days |
Negative Tier Changes
| Tier 1 to Tier 2 | · Naproxen 125mg/5ml susp
· Theophylline 450mg ER tabs |
| Tier 5 to Tier 4 | · Prograf 1mg
· Retacrit inj |
| Tier 2 to Tier 4 | · Sevelamer 800mg tabs |
Prior Authorization Added
| · Alimta inj
· Pemetrexed inj · Zeposia caps |
Please Note: The P&T Committee meets bimonthly and formulary changes and criteria changes can occur during the meetings. Negative formulary changes are made effective on 1/1 and 7/1, while positive formulary changes are effective immediately to better serve our members and providers.
Northwest Pharmacy Updates
All Plans
Neurology
Formulary Additions
- Amvuttra (vutrisiran)—Treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis (hATTR-PN) in adults
- Formulary placement recommendations
- WA Individual—Non-Preferred Specialty Medical with PA
- Medicare—Medicare Part B
- Formulary placement recommendations
- Vabysmo (faricimab-svoa)—Treatment of neovascular (wet) age-related macular degeneration and diabetic macular edema
- Formulary placement recommendations
- WA Individual—Non-Preferred Specialty Medical
- Medicare—Medicare Part B
- Formulary placement recommendations
WA Individual
Neurology
New WA Individual Policies
- Combination Medications for EHB
- Firdapse (amifampridine)
WA Individual Criteria Changes
- Cerdelga (eliglustat tartrate)
- Updated with additional exclusion criteria
- Cerezyme (imiglucerase)
- Added age requirement
- Carbaglu (carglumic acid)
- Added ordering prescriber requirement
- Crysvita (burosumab)
- Added new diagnosis and criteria
- Updated approval period
- Lumizyme (alglucosidase)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Nexviazyme (alglucosidase alfa-ngpt)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Naglazyme (galsulfase)
- Added gene testing requirement
- Mepsevii (vestronidase alfa-vjbk)
- Added exclusions
- Makena (hydroxyprogesterone caproate)
- Added generic to policy
- Added criteria for generic for non-pregnancy related indications
- Onpattro (patisiran)
- Added Amvuttra to policy
- Updated approval period
- Tegsedi (inotersen)
- Added Amvuttra to disallowed concurrent medications
- Enspryng (satralizumab)
- Added exclusion criteria
- Uplizna (inebilizumab)
- Added clarification that Uplizna will not be approved for use in combination with Enspryng or Soliris
- VPRIV (velaglucerase alfa)
- Added Zavesca to disallowed concurrent medications
- Zavesca (miglustat)
- Updated coverage criteria
- Updated age requirement
- Hereditary Angioedema
- Updated Orladeyo MDL
- Spinraza (nusinersen)
- Added medical director review requirement
- Updated approval period
- Vimizim (elosulfase alfa)
- Added required evidence of specific gene mutation
- Kuvan (sapropterin)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Updated approval periods
- Orfadin (nitisinone) and Nityr (nitisinone)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Samsca (tolvaptan)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Syprine (trientine hydrochloride)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Emflaza (deflazacort)
- Updated approval period
- Galafold (migalastat)
- Updated approval period
- Givlaari (givosiran)
- Updated criteria and approval period
- Keveyis (dichlorphenamide)
- Updated approval period
- Oxlumo (lumasiran)
- Updated approval period
- Palynziq (pegvaliase-pqpz)
- Updated approval period
- Revcovi (elapegademase)
- Updated approval period
- Strensiq (asfotase alfa)
- Updated approval period
- Zokinvy (lonafarnib)
- Updated approval period
Additional WA Individual Criteria Changes
- Crohn’s Policy
- Added Skyrizi
- Diabetes Policy
- Removed Mounjaro-specific section and added Mounjaro to GLP-1 section
- Clarified that GLP-1 products will be approved for FDA-approved indications and not solely for weight loss
- Atopic Dermatitis Policy
- Removed Eucrisa step in section 1
- Added step through preferred products in section 2
- Ankylosing Spondylitis Policy
- Added Enbrel to preferred products
- Plaque Psoriasis Policy
- Added Enbrel to preferred products and Sotyku to non-preferred products
- Psoriatic Arthritis Policy
- Added Enbrel to preferred products
- Polyarticular Juvenile Arthritis Policy
- Added Enbrel to preferred products
- Rheumatoid Arthritis Policy
- Added Enbrel to preferred products
Retired Policies
- Korsuva (difelikefalin)
- Will be bundled with other dialysis products
- Ruzurgi (amifampridine)
- Drug is discontinued
Tier Changes
WA Individual
Positive Changes
- Alphagan P: Move from Non-Preferred Brand to Preferred Brand
- Cibinqo: Move from Non-preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Combigan: Move from Non-Preferred brand to Preferred brand
- Simbrinza: Move from Non-Preferred brand to Preferred brand
- Enbrel: Move from Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy (effective 1/1/23)
- Firdapse: Move from Excluded to Non-Preferred Specialty Pharmacy
- Kerendia: Move from Non-Preferred Brand to Preferred Brand
- Lanreotide: Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Mounjaro: Move from Non-Preferred Brand to Preferred Brand
Negative Changes—Effective 1/1/2023
- Betoptic- S: Move from Preferred Brand to Non-Preferred Brand
- Tecfidera: Move from Preferred Specialty Pharmacy to Non-Preferred Specialty Pharmacy
Medicare
Medicare Part D Policies
- New policy: Medicare D Ztalmy
- Criteria changes: Medicare D Skyrizi
- Added criteria and indication for PsA and Crohn’s disease
2023 Medicare Pharmacy Formulary Changes
Positive Changes
Positive Formulary Additions, Increases
| CHANGE | DRUG |
| Addition | Flovent Diskus and Flovent HFA- Tier 4, ST, QL |
| Addition | Gemtesa – Tier 4 |
| MDL increase | Lidocaine/prilocaine cream- increase QL to 60g/30 days **not on initial
formulary for 9/1 Marcom release |
| Addition | Moxifloxacin 400mg tablets- Tier 2 |
| Addition | Ropinirole ER tablets – Tier 2 |
B V D Changes
| B v D removal | Cabenuva susp |
| B v D removal | Duramorph inj |
| B v D removal | Morphine Sul inj 0.5mg/ml, 1mg/ml, 2mg/ml, 4mg/ml |
Positive Tier Changes
| Tier 5 to Tier 3 | · Dalfampridine 10mg ER tabs |
| Tier 2 to Tier 1 | · Klor-Con M15 15meq ER tabs
· Pot cl micro 15meq ER tabs |
Negative Changes
Remove from the Formulary
| Afinitor tablets (no utilization,
generic available) |
Albuterol tablets (discontinued in U.S > 1
year) |
Ambisome inj
(no utilization, generic available) |
Anadrol-50 tabs (discontinued in U.S > 1
year) |
| Aplenzin tabs (remove brand- generic option
available) |
Apokyn inj (remove brand- generic option available) | Apo-Verenicline tablets (remove brand- generic option
available) |
Aptivus solution (discontinued product, capsules still on
formulary) |
| Arcapta caps (discontinued in U.S > 1 year) | Avandia tablets (discontinued in U.S > 1 year) | Azasan tablets (remove brand-no utilization, generic
available) |
Azopt 1% opth susp (remove brand- 1 member, generic
available) |
| Baciim inj (other generic
options available) |
BYNFEZIA PEN INJ 2500MCG
(discontinued product, other generic available) |
Bydureon 2mg inj pen (discontinued product with BCise product
available) |
Bystolic tabs (remove brand, generic available) |
| Captopril/HCTZ tabs (discontinued in U.S > 1 year) | Carbaglu tabs
(remove brand, generic available) |
Chantix pak and tabs (remove brand, no utilization, generic
available) |
Clovique caps (discontinued product, generic available) |
| Crixivan caps (discontinued product) | Cuvposa soln (remove brand, no
utilization, generic available) |
Didanosine caps (discontinued in U.S > 1 year) | Cystadane powd (remove brand, no utilization, generic
available) |
| Diastat gel (remove brand, no utilization, generic
available) |
Dilantin oral susp (remove brand, no
utilization, generic available) |
Duexis tabs (remove brand, no utilization, generic
available) |
Epaned soln (remove brand, generic available) |
| Epirubicin hcl inj (discontinued product) | Erwinaze inj (discontinued product) | Ferriprox tabs (brand removal, no
utilization, generic available) |
Freamine HBC inj 6.9% (discontinued product,
other generics available) |
| Glycate tabs (remove brand, discontinued product, generic
available) |
Gralise tabs (removed due to pricing, other options available) | Guanidine tabs (discontinued in U.S > 1 year) | Hectorol inj (brand removal, generic available) |
| Hepatamine soln (discontinued product) | Horizant tabs (removed due to pricing, other options available) | Hydrocodone/acetami nophen 10/325mg soln (discontinued
product) |
Intelence 100mg, 200mg tabs (brand removal, no utilization,
generic available NF) |
| Kaletra 100/25mg tabs (no utilization) | Ketoprofen
(IR and ER) caps (no utilization, high cost medication) |
Lanoxin tabs (brand removal, no utilization, generic available) | Lazanda spr (discontinued product) |
| Levorphanol tabs (no utilization, high cost, other alternatives
available) |
Maprotiline tabs (discontinued product) | Mondoxyne NL caps (product discontinued, other generic alternatives available) | Morgidox caps (product discontinued, other generic alternatives available) |
| Namenda XR caps (brand removal, generic alternative
available) |
Nephramine inj (discontinued product) | Nitrostat sl tabs (brand removal, generic available) | Northera caps (brand removal, no utilization, generic
available) |
| Oxycodone/ASA tabs (discontinued in U.S > 1 year) | Pacerone tabs (brand removal, generic available) | Paxil susp
(brand removal, no utilization, generic available) |
PEG-intron kit (discontinued in U.S > 1 year) |
| Pepaxto inj
(voluntary removal from market) |
Phospholine opth soln. (discontinued product) | Prednicarbate 0.1%
cream (discontinued product) |
Propantheline tabs
(discontinued in U.S > 1 year) |
| Propranolol/HCTZ tabs (discontinued product by 6/23, available
separately) |
Revlimid 5mg, 10mg, 15mg, 25mg (brand removal, generic available) | Riomet ER susp (discontinued product) | Selzentry 150mg, 300mg (brand removal, generic available) |
| Sutent caps (brand removal, generic available) | Tolbutamide tabs (discontinued product) | Tolmetin sod caps (discontinued in U.S > 1 year) | Tremfya inj (switching preferred and non-preferred
products) |
| Trilyte soln (discontinued
product) |
Trokendi XR caps (brand removal, generic available) | Utibron caps (discontinued in U.S >
1 year) |
Virt-Nate DHA caps (discontinued product) |
| Xcopri pak
(250mg daily dose) (discontinued product) |
Xpovio pak
(100mg and 40mg packs) (discontinued products) |
Zortress tabs (brand removal, no
utilization, generic available) |
Quantity Limits Added
| Dextroamphetamine 5mg/5ml soln- 1800/30 days |
| Linezolid 100mg/5ml susp- add 1800/30 days |
| Mayzent 0.25mg tabs- 120 per 30 days |
| Mayzent starter pack 0.25mg – 14 per 365 days |
| Mayzent starter pack 0.25mg – 24 per 365 days |
| Mayzent 1mg tabs – 30 per 30 days |
| Mayzent 2mg tabs – 30 per 30 days |
Negative Tier Changes
| Tier 1 to Tier 2 | · Naproxen 125mg/5ml susp
· Theophylline 450mg ER tabs |
| Tier 5 to Tier 4 | · Prograf 1mg
· Retacrit inj |
| Tier 2 to Tier 4 | · Sevelamer 800mg tabs |
Prior Authorization Added
| · Alimta inj
· Pemetrexed inj · Zeposia caps |
Please Note: The P&T Committee meets bimonthly and formulary changes and criteria changes can occur during the meetings. Negative formulary changes are made effective on 1/1 and 7/1, while positive formulary changes are effective immediately to better serve our members and providers.
Carle Pharmacy Updates
All Plans
Neurology
Formulary Additions
- Amvuttra (vutrisiran)—Treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis (hATTR-PN) in adults
- Formulary placement recommendations
- Commercial—Non-Preferred Specialty Medical with PA
- Medicare—Medicare Part B
- Formulary placement recommendations
- Vabysmo (faricimab-svoa)—Treatment of neovascular (wet) age-related macular degeneration and diabetic macular edema
- Formulary placement recommendations
- Commercial—Non-Preferred Specialty Medical
- Medicare—Medicare Part B
- Formulary placement recommendations
Commercial
Neurology
New Commercial Policies
- Combination Medications for EHB
- Firdapse (amifampridine)
Commercial Criteria Changes
- Cerdelga (eliglustat tartrate)
- Updated with additional exclusion criteria
- Cerezyme (imiglucerase)
- Added age requirement
- Carbaglu (carglumic acid)
- Added ordering prescriber requirement
- Crysvita (burosumab)
- Added new diagnosis and criteria
- Updated approval period
- Lumizyme (alglucosidase)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Nexviazyme (alglucosidase alfa-ngpt)
- Added age and 6 minute walk test to criteria
- Updated approval period
- Naglazyme (galsulfase)
- Added gene testing requirement
- Mepsevii (vestronidase alfa-vjbk)
- Added exclusions
- Makena (hydroxyprogesterone caproate)
- Added generic to policy
- Added criteria for generic for non-pregnancy related indications
- Onpattro (patisiran)
- Added Amvuttra to policy
- Updated approval period
- Tegsedi (inotersen)
- Added Amvuttra to disallowed concurrent medications
- Enspryng (satralizumab)
- Added exclusion criteria
- Uplizna (inebilizumab)
- Added clarification that Uplizna will not be approved for use in combination with Enspryng or Soliris
- VPRIV (velaglucerase alfa)
- Added Zavesca to disallowed concurrent medications
- Zavesca (miglustat)
- Updated coverage criteria
- Updated age requirement
- Hereditary Angioedema
- Updated Orladeyo MDL
- Spinraza (nusinersen)
- Added medical director review requirement
- Updated approval period
- Vimizim (elosulfase alfa)
- Added required evidence of specific gene mutation
- Kuvan (sapropterin)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Updated approval periods
- Orfadin (nitisinone) and Nityr (nitisinone)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Samsca (tolvaptan)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Syprine (trientine hydrochloride)
- Added generic to policy
- Added generic trial and failure requirement for brand
- Emflaza (deflazacort)
- Updated approval period
- Galafold (migalastat)
- Updated approval period
- Givlaari (givosiran)
- Updated criteria and approval period
- Keveyis (dichlorphenamide)
- Updated approval period
- Oxlumo (lumasiran)
- Updated approval period
- Palynziq (pegvaliase-pqpz)
- Updated approval period
- Revcovi (elapegademase)
- Updated approval period
- Strensiq (asfotase alfa)
- Updated approval period
- Zokinvy (lonafarnib)
- Updated approval period
Additional Commercial Criteria Changes
- Crohn’s Policy
- Added Skyrizi
- Diabetes Policy
- Removed Mounjaro-specific section and added Mounjaro to GLP-1 section
- Clarified that GLP-1 products will be approved for FDA-approved indications and not solely for weight loss
- Atopic Dermatitis Policy
- Removed Eucrisa step in section 1
- Added step through preferred products in section 2
- Ankylosing Spondylitis Policy
- Added Enbrel to preferred products
- Plaque Psoriasis Policy
- Added Enbrel to preferred products and Sotyku to non-preferred products
- Psoriatic Arthritis Policy
- Added Enbrel to preferred products
- Polyarticular Juvenile Arthritis Policy
- Added Enbrel to preferred products
- Rheumatoid Arthritis Policy
- Added Enbrel to preferred products
Retired Policies
- Korsuva (difelikefalin)
- Will be bundled with other dialysis products
- Ruzurgi (amifampridine)
- Drug is discontinued
Tier Changes
Commercial
Positive Changes
- Alphagan P: Move from Non-Preferred Brand to Preferred Brand
- Cibinqo: Move from Non-preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Combigan: Move from Non-Preferred brand to Preferred brand
- Simbrinza: Move from Non-Preferred brand to Preferred brand
- Enbrel: Move from Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy (effective 1/1/23)
- Firdapse: Move from Excluded to Non-Preferred Specialty Pharmacy
- Kerendia: Move from Non-Preferred Brand to Preferred Brand
- Lanreotide: Non-Preferred Specialty Pharmacy to Preferred Specialty Pharmacy
- Mounjaro: Move from Non-Preferred Brand to Preferred Brand
Negative Changes—Effective 1/1/2023
- Betoptic- S: Move from Preferred Brand to Non-Preferred Brand
- Tecfidera: Move from Preferred Specialty Pharmacy to Non-Preferred Specialty Pharmacy
Medicare
Medicare Part D Policies
- New policy: Medicare D Ztalmy
- Criteria changes: Medicare D Skyrizi
- Added criteria and indication for PsA and Crohn’s disease
2023 Medicare Pharmacy Formulary Changes
Positive Changes
Positive Formulary Additions, Increases
| CHANGE | DRUG |
| Addition | Flovent Diskus and Flovent HFA- Tier 4, ST, QL |
| Addition | Gemtesa – Tier 4 |
| MDL increase | Lidocaine/prilocaine cream- increase QL to 60g/30 days **not on initial
formulary for 9/1 Marcom release |
| Addition | Moxifloxacin 400mg tablets- Tier 2 |
| Addition | Ropinirole ER tablets – Tier 2 |
B V D Changes
| B v D removal | Cabenuva susp |
| B v D removal | Duramorph inj |
| B v D removal | Morphine Sul inj 0.5mg/ml, 1mg/ml, 2mg/ml, 4mg/ml |
Positive Tier Changes
| Tier 5 to Tier 3 | · Dalfampridine 10mg ER tabs |
| Tier 2 to Tier 1 | · Klor-Con M15 15meq ER tabs
· Pot cl micro 15meq ER tabs |
Negative Changes
Remove from the Formulary
| Afinitor tablets (no utilization,
generic available) |
Albuterol tablets (discontinued in U.S > 1
year) |
Ambisome inj
(no utilization, generic available) |
Anadrol-50 tabs (discontinued in U.S > 1
year) |
| Aplenzin tabs (remove brand- generic option
available) |
Apokyn inj (remove brand- generic option available) | Apo-Verenicline tablets (remove brand- generic option
available) |
Aptivus solution (discontinued product, capsules still on
formulary) |
| Arcapta caps (discontinued in U.S > 1 year) | Avandia tablets (discontinued in U.S > 1 year) | Azasan tablets (remove brand-no utilization, generic
available) |
Azopt 1% opth susp (remove brand- 1 member, generic
available) |
| Baciim inj (other generic
options available) |
BYNFEZIA PEN INJ 2500MCG
(discontinued product, other generic available) |
Bydureon 2mg inj pen (discontinued product with BCise product
available) |
Bystolic tabs (remove brand, generic available) |
| Captopril/HCTZ tabs (discontinued in U.S > 1 year) | Carbaglu tabs
(remove brand, generic available) |
Chantix pak and tabs (remove brand, no utilization, generic
available) |
Clovique caps (discontinued product, generic available) |
| Crixivan caps (discontinued product) | Cuvposa soln (remove brand, no
utilization, generic available) |
Didanosine caps (discontinued in U.S > 1 year) | Cystadane powd (remove brand, no utilization, generic
available) |
| Diastat gel (remove brand, no utilization, generic
available) |
Dilantin oral susp (remove brand, no
utilization, generic available) |
Duexis tabs (remove brand, no utilization, generic
available) |
Epaned soln (remove brand, generic available) |
| Epirubicin hcl inj (discontinued product) | Erwinaze inj (discontinued product) | Ferriprox tabs (brand removal, no
utilization, generic available) |
Freamine HBC inj 6.9% (discontinued product,
other generics available) |
| Glycate tabs (remove brand, discontinued product, generic
available) |
Gralise tabs (removed due to pricing, other options available) | Guanidine tabs (discontinued in U.S > 1 year) | Hectorol inj (brand removal, generic available) |
| Hepatamine soln (discontinued product) | Horizant tabs (removed due to pricing, other options available) | Hydrocodone/acetami nophen 10/325mg soln (discontinued
product) |
Intelence 100mg, 200mg tabs (brand removal, no utilization,
generic available NF) |
| Kaletra 100/25mg tabs (no utilization) | Ketoprofen
(IR and ER) caps (no utilization, high cost medication) |
Lanoxin tabs (brand removal, no utilization, generic available) | Lazanda spr (discontinued product) |
| Levorphanol tabs (no utilization, high cost, other alternatives
available) |
Maprotiline tabs (discontinued product) | Mondoxyne NL caps (product discontinued, other generic alternatives available) | Morgidox caps (product discontinued, other generic alternatives available) |
| Namenda XR caps (brand removal, generic alternative
available) |
Nephramine inj (discontinued product) | Nitrostat sl tabs (brand removal, generic available) | Northera caps (brand removal, no utilization, generic
available) |
| Oxycodone/ASA tabs (discontinued in U.S > 1 year) | Pacerone tabs (brand removal, generic available) | Paxil susp
(brand removal, no utilization, generic available) |
PEG-intron kit (discontinued in U.S > 1 year) |
| Pepaxto inj
(voluntary removal from market) |
Phospholine opth soln. (discontinued product) | Prednicarbate 0.1%
cream (discontinued product) |
Propantheline tabs
(discontinued in U.S > 1 year) |
| Propranolol/HCTZ tabs (discontinued product by 6/23, available
separately) |
Revlimid 5mg, 10mg, 15mg, 25mg (brand removal, generic available) | Riomet ER susp (discontinued product) | Selzentry 150mg, 300mg (brand removal, generic available) |
| Sutent caps (brand removal, generic available) | Tolbutamide tabs (discontinued product) | Tolmetin sod caps (discontinued in U.S > 1 year) | Tremfya inj (switching preferred and non-preferred
products) |
| Trilyte soln (discontinued
product) |
Trokendi XR caps (brand removal, generic available) | Utibron caps (discontinued in U.S >
1 year) |
Virt-Nate DHA caps (discontinued product) |
| Xcopri pak
(250mg daily dose) (discontinued product) |
Xpovio pak
(100mg and 40mg packs) (discontinued products) |
Zortress tabs (brand removal, no
utilization, generic available) |
Quantity Limits Added
| Dextroamphetamine 5mg/5ml soln- 1800/30 days |
| Linezolid 100mg/5ml susp- add 1800/30 days |
| Mayzent 0.25mg tabs- 120 per 30 days |
| Mayzent starter pack 0.25mg – 14 per 365 days |
| Mayzent starter pack 0.25mg – 24 per 365 days |
| Mayzent 1mg tabs – 30 per 30 days |
| Mayzent 2mg tabs – 30 per 30 days |
Negative Tier Changes
| Tier 1 to Tier 2 | · Naproxen 125mg/5ml susp
· Theophylline 450mg ER tabs |
| Tier 5 to Tier 4 | · Prograf 1mg
· Retacrit inj |
| Tier 2 to Tier 4 | · Sevelamer 800mg tabs |
Prior Authorization Added
| · Alimta inj
· Pemetrexed inj · Zeposia caps |
Please Note: The P&T Committee meets bimonthly and formulary changes and criteria changes can occur during the meetings. Negative formulary changes are made effective on 1/1 and 7/1, while positive formulary changes are effective immediately to better serve our members and providers.
Reid Pharmacy Updates
Medicare
Neurology
Formulary Additions
- Amvuttra (vutrisiran)—Treatment of the polyneuropathy of hereditary transthyretin-mediated amyloidosis (hATTR-PN) in adults
- Formulary placement recommendations
- Medicare—Medicare Part B
- Formulary placement recommendations
- Vabysmo (faricimab-svoa)—Treatment of neovascular (wet) age-related macular degeneration and diabetic macular edema
- Formulary placement recommendations
- Medicare—Medicare Part B
- Formulary placement recommendations
Medicare Part D Policies
- New policy: Medicare D Ztalmy
- Criteria changes: Medicare D Skyrizi
- Added criteria and indication for PsA and Crohn’s disease
2023 Medicare Pharmacy Formulary Changes
Positive Changes
Positive Formulary Additions, Increases
| CHANGE | DRUG |
| Addition | Flovent Diskus and Flovent HFA- Tier 4, ST, QL |
| Addition | Gemtesa – Tier 4 |
| MDL increase | Lidocaine/prilocaine cream- increase QL to 60g/30 days **not on initial
formulary for 9/1 Marcom release |
| Addition | Moxifloxacin 400mg tablets- Tier 2 |
| Addition | Ropinirole ER tablets – Tier 2 |
B V D Changes
| B v D removal | Cabenuva susp |
| B v D removal | Duramorph inj |
| B v D removal | Morphine Sul inj 0.5mg/ml, 1mg/ml, 2mg/ml, 4mg/ml |
Positive Tier Changes
| Tier 5 to Tier 3 | · Dalfampridine 10mg ER tabs |
| Tier 2 to Tier 1 | · Klor-Con M15 15meq ER tabs
· Pot cl micro 15meq ER tabs |
Negative Changes
Remove from the Formulary
| Afinitor tablets (no utilization,
generic available) |
Albuterol tablets (discontinued in U.S > 1
year) |
Ambisome inj
(no utilization, generic available) |
Anadrol-50 tabs (discontinued in U.S > 1
year) |
| Aplenzin tabs (remove brand- generic option
available) |
Apokyn inj (remove brand- generic option available) | Apo-Verenicline tablets (remove brand- generic option
available) |
Aptivus solution (discontinued product, capsules still on
formulary) |
| Arcapta caps (discontinued in U.S > 1 year) | Avandia tablets (discontinued in U.S > 1 year) | Azasan tablets (remove brand-no utilization, generic
available) |
Azopt 1% opth susp (remove brand- 1 member, generic
available) |
| Baciim inj (other generic
options available) |
BYNFEZIA PEN INJ 2500MCG
(discontinued product, other generic available) |
Bydureon 2mg inj pen (discontinued product with BCise product
available) |
Bystolic tabs (remove brand, generic available) |
| Captopril/HCTZ tabs (discontinued in U.S > 1 year) | Carbaglu tabs
(remove brand, generic available) |
Chantix pak and tabs (remove brand, no utilization, generic
available) |
Clovique caps (discontinued product, generic available) |
| Crixivan caps (discontinued product) | Cuvposa soln (remove brand, no
utilization, generic available) |
Didanosine caps (discontinued in U.S > 1 year) | Cystadane powd (remove brand, no utilization, generic
available) |
| Diastat gel (remove brand, no utilization, generic
available) |
Dilantin oral susp (remove brand, no
utilization, generic available) |
Duexis tabs (remove brand, no utilization, generic
available) |
Epaned soln (remove brand, generic available) |
| Epirubicin hcl inj (discontinued product) | Erwinaze inj (discontinued product) | Ferriprox tabs (brand removal, no
utilization, generic available) |
Freamine HBC inj 6.9% (discontinued product,
other generics available) |
| Glycate tabs (remove brand, discontinued product, generic
available) |
Gralise tabs (removed due to pricing, other options available) | Guanidine tabs (discontinued in U.S > 1 year) | Hectorol inj (brand removal, generic available) |
| Hepatamine soln (discontinued product) | Horizant tabs (removed due to pricing, other options available) | Hydrocodone/acetami nophen 10/325mg soln (discontinued
product) |
Intelence 100mg, 200mg tabs (brand removal, no utilization,
generic available NF) |
| Kaletra 100/25mg tabs (no utilization) | Ketoprofen
(IR and ER) caps (no utilization, high cost medication) |
Lanoxin tabs (brand removal, no utilization, generic available) | Lazanda spr (discontinued product) |
| Levorphanol tabs (no utilization, high cost, other alternatives
available) |
Maprotiline tabs (discontinued product) | Mondoxyne NL caps (product discontinued, other generic alternatives available) | Morgidox caps (product discontinued, other generic alternatives available) |
| Namenda XR caps (brand removal, generic alternative
available) |
Nephramine inj (discontinued product) | Nitrostat sl tabs (brand removal, generic available) | Northera caps (brand removal, no utilization, generic
available) |
| Oxycodone/ASA tabs (discontinued in U.S > 1 year) | Pacerone tabs (brand removal, generic available) | Paxil susp
(brand removal, no utilization, generic available) |
PEG-intron kit (discontinued in U.S > 1 year) |
| Pepaxto inj
(voluntary removal from market) |
Phospholine opth soln. (discontinued product) | Prednicarbate 0.1%
cream (discontinued product) |
Propantheline tabs
(discontinued in U.S > 1 year) |
| Propranolol/HCTZ tabs (discontinued product by 6/23, available
separately) |
Revlimid 5mg, 10mg, 15mg, 25mg (brand removal, generic available) | Riomet ER susp (discontinued product) | Selzentry 150mg, 300mg (brand removal, generic available) |
| Sutent caps (brand removal, generic available) | Tolbutamide tabs (discontinued product) | Tolmetin sod caps (discontinued in U.S > 1 year) | Tremfya inj (switching preferred and non-preferred
products) |
| Trilyte soln (discontinued
product) |
Trokendi XR caps (brand removal, generic available) | Utibron caps (discontinued in U.S >
1 year) |
Virt-Nate DHA caps (discontinued product) |
| Xcopri pak
(250mg daily dose) (discontinued product) |
Xpovio pak
(100mg and 40mg packs) (discontinued products) |
Zortress tabs (brand removal, no
utilization, generic available) |
Quantity Limits Added
| Dextroamphetamine 5mg/5ml soln- 1800/30 days |
| Linezolid 100mg/5ml susp- add 1800/30 days |
| Mayzent 0.25mg tabs- 120 per 30 days |
| Mayzent starter pack 0.25mg – 14 per 365 days |
| Mayzent starter pack 0.25mg – 24 per 365 days |
| Mayzent 1mg tabs – 30 per 30 days |
| Mayzent 2mg tabs – 30 per 30 days |
Negative Tier Changes
| Tier 1 to Tier 2 | · Naproxen 125mg/5ml susp
· Theophylline 450mg ER tabs |
| Tier 5 to Tier 4 | · Prograf 1mg
· Retacrit inj |
| Tier 2 to Tier 4 | · Sevelamer 800mg tabs |
Prior Authorization Added
| · Alimta inj
· Pemetrexed inj · Zeposia caps |
Please Note: The P&T Committee meets bimonthly and formulary changes and criteria changes can occur during the meetings. Negative formulary changes are made effective on 1/1 and 7/1, while positive formulary changes are effective immediately to better serve our members and providers.
Contact Us
(800) 851-3379, option 3